Weather fluctuations: predictive factors in the prevalence of acute coronary syndrome
Health Promotion Perspectives, 9(2), 123-130; DOI:10.15171/hpp.2019.17
Original Article
Weather fluctuations: predictive factors in the prevalence of acute coronary syndrome
Hamid Sharif Nia1, Yiong Huak Chan2, Erika Sivarajan Froelicher3, Saeed Pahlevan Sharif4, Ameneh Yaghoobzadeh5, Azar Jafari6, Amir Hossein Goudarzian7 ,*, Roghiyeh Pourkia8, Ali Akbar Haghdoost9, Farhad Arefinia10, Roghieh Nazari1
1
Department of Medical-Surgical Nursing, School of Nursing and Midwifery Amol, Mazandaran University of Medical Sciences, Sari, Iran
2
Biostatistics Unit, Yong Loo Lin School of Medicine, National University Health System, Singapore
3
Department of Physiological Nursing, Department of Epidemiology & Biostatistics, University of California San Francisco, California, USA
4
Taylor’s Business School, Taylor’s University Malaysia, Subang Jaya, Malaysia
5
Department of Nursing, Tehran University of Medical Sciences, Tehran, Iran
6
Department of Nursing, Mazandaran University of Medical Sciences, Sari, Iran
7
Faculty of Nursing, Student Research Committee, Mazandaran University of Medical Sciences, Sari, Iran
8
Department of Cardiology, Cardiovascular Research Center, Babol University of Medical Sciences, Babol, Iran
9
Modeling in Health Research Center, Institute for Futures Studies in Health, Kerman University of Medical Sciences, Kerman, Iran
10
School of Nursing and Midwifery Amol, Mazandaran University of Medical Sciences, Sari, Iran
Email: amir_sari@yahoo.com
© 2019 The Author(s). This is an open access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background: Meteorological parameters and seasonal changes can play an important role in the occurrence of acute coronary syndrome (ACS). However, there is almost no evidence on a national level to suggest the associations between these variables and ACS in Iran. We aim to identify the meteorological parameters and seasonal changes in relationship to ACS.
Methods: This retrospective cross-sectional study was conducted between 03/19/2015 to 03/18/2016 and used documents and records of patients with ACS in Mazandaran ProvinceHeart Center, Iran. The following definitive diagnostic criteria for ACS were used: (1) existence of cardiac enzymes (CK or CK-MB) above the normal range; (2) Greater than 1 mm ST-segment elevation or depression; (3) abnormal Q waves; and (4) manifestation of troponin enzyme in the blood. Data were collected daily, such as temperature (Celsius) changes, wind speed and its direction, rainfall, daily evaporation rate; number of sunny days, and relative humidity were provided by the Meteorological Organization of Iran.
Results: A sample of 2,054 patients with ACS were recruited. The results indicated the highest ACS events from March to May. Generally, wind speed (18 PM) [IRR = 1.051 (95% CI: 1.019 to1.083), P=0.001], daily evaporation [IRR = 1.039 (95% CI: 1.003 to 1.077), P=0.032], daily maximum (P<0.001) and minimum (P=0.003) relative humidity was positively correlated withACS events. Also, negatively correlated variables were daily relative humidity (18 PM) [IRR =0.985 (95% CI: 0.978 to 0.992), P<0.001], and daily minimum temperature [IRR = 0.942 (95%CI: 0.927 to 0.958), P<0.001].
Conclusion: Climate changes were found to be significantly associated with ACS; especially from cold weather to hot weather in March, April and May. Further research is needed to fully understand the specific conditions and cold exposures.
Keywords: Meteorological parameters, Seasonal changes, Acute coronary syndrome, Prevalence, Iran
Citation: Sharif Nia H, Chan YH, Froelicher ES, Pahlevan Sharif S, Yaghoobzadeh A, Jafari A, et al. Weather fluctuations: predictive factors in the prevalence of acute coronary syndrome. Health Promot Perspect. 2019;9(2):123-130. doi: 10.15171/hpp.2019.17.
Introduction
Acute coronary syndrome (ACS) is one of the most common health problems in the world, which can increase mental health problems, result in considerable disability, increase morbidity, and mortality.1,2 Studies during several decades have focused on different pathophysiological mechanisms and predisposing factors for the incidence of ACS.3-5 One of these studies focused on the effects of weather conditions on incidence of ACS that has been discussed in different areas of the world for more than 50 years.6 A number of investigators found that meteorological parameters and seasonal changes can play an important role in the occurrence of ACS.7,8 The role of temperature is both direct and fast. Time series studies have revealed that there is a minimum lag time of about 24 hours between decrease in temperature and increase in mortality.9 The study reported that approximately 4% of ACS onsets are associated with different kinds of meteorological parameters.10 In another study, it was found that weather conditions like atmospheric air temperature, humidity, wind speed, and wind pressure effects the incidence of ACS.11-13 Although several studies suggest that ACS occurs most often in the winter months,14-17 other studies report that the occurrence rate of ACS increases in spring.6,18 Yet another study shows that ACS occurs in summer when the temperature and humidity are high and atmospheric pressure is low.19 It has also been shown that there is an association between temperature, high relative humidity, and strong winds and ACS.9 It seems that physiologic stressors such as sympathetic activation, hypercoagulability and infection in cold weather condition (such as influenza epidemics and air pollution) are linked to the incidence of ACS.20 Additionally, hemodynamic changes are exacerbated during winter, as are elevated immune reactions, uncontrolled hypertension, immobility, and risk for respiratory infections,21 that can affect the incidence of ACS. Some studies state that cold temperature effects platelet numbers, arterial blood pressure, and thrombus formation.19 Also, variation of incidence of ACS in different seasons is attributed to variability in ultraviolet-B exposure during the seasons and vitamin D deficiency that may increase the cardiovascular risk.22 Nevertheless, a 1°C decrease in temperature caused a 1%–2% rise in the number of deaths.9
Although numerous studies have been conducted on the impact of climate variables and seasonal changes on the risk of ACS in different areas of the world; many of these studies lack national level data. However, there is almost no evidence to suggest an association between climate variables and the risk of ACS in Iran. So, due to the importance of reducing the incidence of ACS and its effects on quality of life, it is important to study the impact of meteorological parameters and seasonal changes on the incidence of ACS in a region with different weather conditions and great geographic diversity. In other words, a better understanding of the seasonal changes may provide novel pathways to prevent ACS.23 Therefore, the present study aims to determine the relationship between meteorological parameters with the incidence of ACS.
Materials and Methods
This retrospective cross-sectional study design was used. This study is based on medical records of the Heart Center of Mazandaran province, Iran. This center provides the most comprehensive data in northern Iran on all patients with a diagnosis of ACS.
Setting
The Mazandaran Province Heart Center, Iran located at the following coordinates (36.369 N, 52.270 W) was chosen because it offers the most complete data in Iran about patients diagnosed with ACS.24 Census sampling method was used. Existing date was used between 03/19/2015 to 03/18/2016. Sari (the capital of Mazandaran) is a north city of Iran which has mild weather. Based on the newest census in 2016, it contains the 505 000 inhabitants. The center consists of five CCU wards, one ICU, and one emergency ward. Registered data of the ACS patients surveyed are used from these units.
Study population
The current study was carried out among all patients referred to the hospital with symptoms of ACS. The cardiologist, two nurses, a statistician, and an epidemiologist (who extracted and recorded the needed information using a data collection guide) formed the research team. The final diagnosis of ACS was verified by the cardiologist. The following were considered as the definitive diagnostic criteria were: (1) existence of cardiac enzymes (CK or CK-MB) above the normal range; (2) ST-segment elevation or depression of more than 1; (3) abnormal Q waves; and (4) manifestation of Troponin enzyme in the blood.2
Two nurses invited patients to participate in the study after the ethical approval of the study had been obtained from the Mazandaran University of Medical Sciences.
Measurements
The following variables were abstracted: gender, the day, month, year and time of hospital admission. Also, weather variables were included daily temperature (Celsius) changes (minimum, maximum, and average), wind speed (meters per second) and its direction, rainfall (day), daily evaporation rate (mm), number of sunny days, and relative humidity (percent) between March 2015 to March 2016 were provided by the Meteorological Organization of Iran. Iran’s four climate seasons are: spring (April to June), summer (July to September), autumn (September to December) and winter (January to March).
Statistical analysis
All analyses were performed using SPSS 24.0 (SPSS 24.0, Inc., Chicago, Illinois, USA) with statistical significance set at α = 0.05. Mean (SD) were presented for numeric normal variables, median (range) for numeric non-normal variables and frequency (%) for categorical variables. General Linear Model was performed to compare the number of ACS events across months adjusting for age, gender and meteorological variables with Bonferroni correction for pairwise comparisons. A negative binomial regression model accounting for over-dispersion was used to determine the meteorological (daily temperature (minimum, maximum, and average), wind speed and its direction, rainfall, daily evaporation rate, number of sunny days, and relative humidity) and demographical predictors on daily (defining a day from 00:00 to 23:59 hours) relative risk (RR) ACS prevalence with a 95% confidence interval, gender-subgroup analyses was also performed.
Results
Sample characteristics
Over the study period, a total of 2054 patients with ACS were recruited. The mean (±SD) age of the subjects was 55.6 (±13.4), median 58 and their ages ranged from 20 to 91 years old, with 49.3% being men. The ages for men were mean (±SD) 56.3 (±13.3), median 58, ranging between 20-91 and 55.0 (±13.5), 57, 20-91 for women. Table 1 shows the descriptive statistics for the meteorological variables.
|
Table 1. Meteorological variables descriptive
|
|
Variable
|
Mean (SD)
|
Range
|
Median
|
| Wind speed |
4.62 (2.36) |
0–20 |
4.0 |
| Wind speed (18 PM) |
1.23 (1.71) |
0–18 |
0.0 |
| Wind speed (12 MD) |
2.22 (1.67) |
0–8 |
2.0 |
| Wind speed (6 AM) |
0.72 (1.26) |
0–8 |
0.0 |
| Daily evaporation |
2.79 (2.27) |
0–9.6 |
2.2 |
| Daily rain |
1.62 (5.68) |
0–69.9 |
0.0 |
| Daily relative humidity (18 pm) |
79.57 (11.75) |
26–98 |
82.0 |
| Daily Relative humidity (12 md) |
66.15 (15.98) |
26–100 |
64.0 |
| Daily Relative humidity (6 am) |
89.42 (9.14) |
30–100 |
92.0 |
| Daily average relative humidity |
78.03 (9.39) |
47.5–98.5 |
78.0 |
| Daily maximum relative humidity |
95.11 (4.33) |
72–100 |
97.0 |
| Daily minimum relative humidity |
60.95 (16.65) |
23–97 |
60.0 |
| Daily average temperature |
16.71 (7.06) |
5.5–33.3 |
15.0 |
| Maximum daily temperature |
21.36 (7.99) |
7.4–42.6 |
19.6 |
Weather fluctuations
Figures 1 and 2 show the number of ACS events by gender and by age in quartiles for each month, respectively.

Figure 1. Number of AMI events by gender over month.
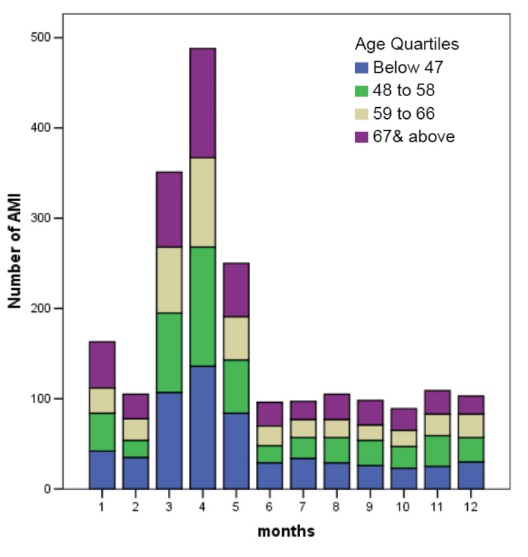
Figure 2. Number of AMI events by age quartiles over month.
Figures 1 and 2 show that the third to the fifth months had statistically higher (P < 0.001) occurrences of ACS events during the year. Overall the other months except for month 5 over month 1 (P = 0.581) adjusting for demographical and meteorological variables with Bonferroni correction (see Table 2).
|
Table 2. Comparison of ACS by month adjusted for age, meteorological variables and sex
|
|
Reference
|
Month
|
Mean Difference (Reference-Month)
|
95% Confidence Interval for Difference
|
Bonferroni corrected
P
value
|
|
|
|
Lower
|
Upper
|
|
| Month 1 |
2 |
58 |
-6.1 |
122.1 |
0.152 |
|
3 |
-188 |
-276.4 |
-99.6 |
< 0.001 |
|
4 |
-325 |
-428.1 |
-221.9 |
< 0.001 |
|
5 |
-87 |
-198.3 |
24.3 |
0.561 |
|
6 |
67 |
-29.3 |
163.3 |
1.000 |
|
7 |
66 |
-34.7 |
166.7 |
1.000 |
|
8 |
58 |
-44.8 |
160.8 |
1.000 |
|
9 |
65 |
-29.7 |
159.7 |
1.000 |
|
10 |
74 |
-6.0 |
154.0 |
0.122 |
|
11 |
54 |
-13.1 |
121.1 |
0.445 |
|
12 |
60 |
-3.3 |
123.3 |
0.092 |
| Month 2 |
3 |
-246 |
-333.0 |
-159.0 |
< 0.001 |
|
4 |
-383 |
-477.9 |
-288.1 |
< 0.001 |
|
5 |
-145 |
-235.3 |
-54.7 |
< 0.001 |
|
6 |
9 |
-64.7 |
82.7 |
1.000 |
|
7 |
8 |
-70.2 |
86.2 |
1.000 |
|
8 |
0 |
-80.2 |
80.2 |
1.000 |
|
9 |
7 |
-65.9 |
79.9 |
1.000 |
|
10 |
16 |
-43.0 |
75.0 |
1.000 |
|
11 |
-4 |
-56.4 |
48.4 |
1.000 |
|
12 |
2 |
-47.8 |
51.8 |
1.000 |
| Month 3 |
4 |
-137 |
-257.1 |
-16.9 |
0.008 |
|
5 |
101 |
-31.9 |
233.9 |
0.690 |
|
6 |
255 |
133.6 |
376.4 |
< 0.001 |
|
7 |
254 |
128.1 |
379.9 |
< 0.001 |
|
8 |
246 |
117.1 |
374.9 |
< 0.001 |
|
9 |
253 |
131.7 |
374.3 |
< 0.001 |
|
10 |
262 |
154.8 |
369.2 |
< 0.001 |
|
11 |
242 |
148.2 |
335.8 |
< 0.001 |
|
12 |
248 |
159.5 |
336.5 |
< 0.001 |
| Month 4 |
5 |
238 |
116.7 |
359.3 |
< 0.001 |
|
6 |
392 |
281.4 |
502.6 |
< 0.001 |
|
7 |
391 |
277.9 |
504.1 |
< 0.001 |
|
8 |
383 |
269.9 |
496.1 |
< 0.001 |
|
9 |
390 |
281.9 |
498.1 |
< 0.001 |
|
10 |
399 |
299.9 |
498.1 |
< 0.001 |
|
11 |
379 |
282.8 |
475.2 |
< 0.001 |
|
12 |
385 |
290.1 |
479.9 |
< 0.001 |
| Month 5 |
6 |
154 |
87.2 |
220.8 |
< 0.001 |
|
7 |
153 |
84.0 |
222.0 |
< 0.001 |
|
8 |
145 |
75.9 |
214.1 |
< 0.001 |
|
9 |
152 |
81.7 |
222.3 |
< 0.001 |
|
10 |
161 |
87.5 |
234.5 |
< 0.001 |
|
11 |
141 |
53.4 |
228.6 |
< 0.001 |
|
12 |
147 |
56.4 |
237.6 |
< 0.001 |
| Month 6 |
7 |
-1 |
-50.8 |
48.8 |
1.000 |
|
8 |
-9 |
-59.5 |
41.5 |
1.000 |
|
9 |
-2 |
-52.2 |
48.2 |
1.000 |
|
10 |
7 |
-46.8 |
60.8 |
1.000 |
|
11 |
-13 |
-82.4 |
56.4 |
1.000 |
|
12 |
-7 |
-80.3 |
66.3 |
1.000 |
| Month 7 |
8 |
-8 |
-58.8 |
42.8 |
1.000 |
|
9 |
-1 |
-51.5 |
49.5 |
1.000 |
|
10 |
8 |
-48.1 |
64.1 |
1.000 |
|
11 |
-12 |
-85.4 |
61.4 |
1.000 |
|
12 |
-6 |
-83.4 |
71.4 |
1.000 |
| Month 8 |
9 |
7 |
-43.2 |
57.2 |
1.000 |
|
10 |
16 |
-39.9 |
71.9 |
1.000 |
|
11 |
-4 |
-79.5 |
71.5 |
1.000 |
|
12 |
2 |
-77.4 |
81.4 |
1.000 |
| Month 9 |
10 |
9 |
-42.3 |
60.3 |
1.000 |
|
11 |
-11 |
-78.7 |
56.7 |
1.000 |
|
12 |
-5 |
-76.5 |
66.5 |
1.000 |
| Month 10 |
11 |
-20 |
-76.1 |
36.1 |
1.000 |
|
12 |
-14 |
-72.0 |
44.0 |
1.000 |
| Month 11 |
12 |
6 |
-44.8 |
56.8 |
1.000 |
|
General Linear Model performed.
|
Factors associated with ACS
Table 3 shows that the variables that were positively correlated with ACS events were wind speed (18 PM), daily evaporation, maximum and minimum relative humidity. Negatively correlated variables were daily relative humidity (6 PM). The analysis by gender shows that for men positive correlates were daily evaporation and daily maximum relative humidity, trend relationship with wind speed (18 PM). For women, wind speed (18 PM), daily minimum and maximum relative humidity were positive correlates; with daily relative humidity (18 PM) and minimum daily temperature negatively correlated with ACS events.
|
Table 3. Predictors for acute coronary syndrome
|
|
Variable
|
IRR (95% CI)
|
P
value
|
|
All subjects
|
| Male mean (SD): 6.13 (5.70) |
1.03 (0.94 to 1.12) |
0.598 |
| Female mean (SD): 5.70 (5.10) |
1.0 |
|
| Age |
1.001 (0.997 to 1.004) |
0.749 |
| Wind speed (18 PM) |
1.051 (1.019 to 1.083) |
0.001 |
| Wind speed (12 MD) |
0.982 (0.953 to 1.011) |
0.220 |
| Wind speed (6 AM) |
1.009 (0.970 to 1.050) |
0.653 |
| Daily evaporation |
1.039 (1.003 to 1.077) |
0.032 |
| Daily rain |
0.992 (0.985 to 1.00) |
0.060 |
| Daily relative humidity (18 PM) |
0.985 (0.978 to 0.992) |
< 0.001 |
| Daily Relative humidity (12 MD) |
0.998 (0.990 to 1.007) |
0.683 |
| Daily maximum relative humidity |
1.036 (1.023 to 1.050) |
< 0.001 |
| Daily minimum relative humidity |
1.013 (1.004 to 1.022) |
0.003 |
| Maximum daily temperature |
1.015 (0.997 to 1.034) |
0.100 |
| Minimum daily temperature |
0.942 (0.927 to 0.958) |
< 0.001 |
|
Males
|
| Age |
1.002 (0.997 to 1.007) |
0.474 |
| Wind speed (18PM) |
1.039 (0.997 to 1.083) |
0.067 |
| Wind speed (12MD) |
0.977 (0.937 to 1.020) |
0.291 |
| Wind speed (6AM) |
1.015 (0.960 to 1.073) |
0.612 |
| Daily evaporation |
1.056 (1.003 to 1.112) |
0.039 |
| Daily rain |
0.991 (0.980 to 1.003) |
0.133 |
| Daily relative humidity (18PM) |
0.990 (0.981 to 1.000) |
0.060 |
| Daily Relative humidity (12MD) |
0.998 (0.987 to 1.010) |
0.786 |
| Daily maximum relative humidity |
1.035 (1.016 to 1.054) |
< 0.001 |
| Daily minimum relative humidity |
1.009 (0.997 to 1.022) |
0.144 |
| Maximum daily temperature |
1.011 (0.984 to 1.037) |
0.430 |
| Minimum daily temperature |
0.945 (0.921 to 0.968) |
< 0.001 |
|
Females
|
| Age |
0.999 (0.995 to 1.004) |
0.756 |
| Wind speed (18PM) |
1.065 (1.019 to 1.114) |
0.006 |
| Wind speed (12MD) |
0.986 (0.947 to 1.028) |
0.508 |
| Wind speed (6AM) |
0.998 (0.944 to 1.050) |
0.941 |
| Daily evaporation |
1.023 (0.975 to 1.055) |
0.356 |
| Daily rain |
0.993 (0.983 to 1.004) |
0.220 |
| Daily relative humidity (18PM) |
0.978 (0.968 to 0.988) |
< 0.001 |
| Daily Relative humidity (12MD) |
0.999 (0.987 to 1.011) |
0.849 |
| Daily maximum relative humidity |
1.038 (1.020 to 1.057) |
< 0.001 |
| Daily minimum relative humidity |
1.017 (1.005 to 1.030) |
0.006 |
| Maximum daily temperature |
1.021 (0.996 to 1.048) |
0.106 |
| Minimum daily temperature |
0.939 (0.917 to 0.961) |
< 0.001 |
|
Negative Binomial regression performed.
Abbreviations: IRR, incident relative risk; CI, confidence interval.
|
Discussion
The study aimed to evaluate the meteorological parameters and seasonal changes in relationship with incidence of ACS; as well as to identify gender differences. The results indicated that ACS admissions were higher March through May. Similarly March was reported as the month with the highest incidence of ACS in Germany.25 However, January was reported to have the highest incidence in the United Sates.17 Other studies found that the incidence and fatality risk of ACS were higher in the winter and spring.4,16,18,20,26-30 However, two additional studies reported that ACS was more common in summer.31,32 There are several mechanisms of climate changes that are suggested for the two pathological exogenous and endogenous responses. Lipid serum level, coagulation systems, and hormonal changes are among these features.23 Also, behavioral pattern variations following seasonal changes like changes in diet, physical activity, and psychosocial factors such as mood are considered as the emerging explanations for the high incidence of ACS in these seasons.33 Besides, variation in temperature,34 seasonal pattern occur such as infections like influenza epidemics,35 elevated concentration of fine element air pollution,10 seasonality phenomenon (i.e. winter depression, anxiety, sadness, social withdrawal, sleep disturbances, irritability, etc),10 respiratory tract infections,36 and reduction in the number of solar light hours37 are other proposed factors of the incidence of ACS. Therefore, differences in the patterns of ACS prevalence according to the time of year and changes in ambient climate within the same location may be reasonable explanations. This concept appears to be especially applicable to the regions of the world subjected to four distinct seasons and significantly different winter-to-summer weather conditions.38
The possible role of meteorological variables has been considered throughout the study. The present study confirmed the positive relationships between wind speed and the incidence of ACS. Goerre et al reported the same findings in their study in Switzerland.39 An inverse relationship was noted in the 10-year ecological study in Great Britain40 and a 12 years survey in Kaunas11 reported also negative correlations. However, another study failed to observe any significant relationships.23
It was investigated that relative humidity was among the factors that negatively correlated with the ACS incidences. Our findings concur with those by Abrignani et al,23 Messner et al,41 and Lee et al.42 one findings stated no correlations43 and two others reported positive relationships among these variables.44,45 Moreover, it seems that the presence of high air humidity may hinder swelling and also make it difficult the automatic processes of internal temperature control. Therefore, the respiratory fatigue and heart rate will be increased.23
Data on the role of environmental temperature are conflicting. One of the remarkable results of the present study was the negative association between daily minimum temperature and the hospital admission due to ACS; this suggests that the daily minimum temperature has a protective role in ACS. In other words, when the temperature is at lowest, it reduced ACS by 6 percent. Some studies indicated that the number of ACS are linked with the both colder and warmer temperatures.44,46,47 A 9-year survey (i.e. 2000-2009) in Hong Kong and Taiwan indicated that the lower mean temperature was associated with lower ACS risk on the same day.7 However, Kysely et al48 and Näyhä49 believe that fatality related to cold or heat is certainly not affected by hypo or hyperthermia. Also, Stewart et al reported that there is some evidence showing cold adaptation through longer exposure to the cold weather may occur. However, this approach is debatable.38 Also reduction in acute phase mortality, due to variations, such as earlier diagnosis of infarction, early and aggressive treatment, suitable reperfusion treatment, additional precise delineation of post ACS risk, as well as more suitable treatment of heart failure and mechanical complications after ACS are among the possible factors leading to reduction in morbidity and mortality following ACS.50,51 It also can be caused by indirect effects including cardiovascular disease that is exacerbated by physiological reactions of the man`s body aimed to adapt to the thermal environment.48,49 To the best of our knowledge, there is no study that reported a negative correlation between the minimum daily temperature and ACS incidence. Further research is needed to fully understand the individual conditions and cold exposure.
Given the fact that seasonal weather effects the prevalence, complications and outcomes of ACS, so that patients should modify their lifestyle particularly during the cold months with a diet rich in vitamins (e.g. vitamin D3), modifies activity level, suitable and warm clothes.52
Although the data of the current study have been extracted from the patients referred to the Sari, capital of Mazandaran city, our findings will be generalized to predict the occurrence of ACS in order to take preventive and therapeutic across the southern Caspian Sea. This happening can be due to the two causes; at first, weather characteristics as well as seasonal changes in the southern parts of the Caspian Sea follow relatively similar pattern53 and the next is that the residents of these areas are prone to vulnerability because of high population density.54
Limitation
Similar to most studies, this study had several limitations: (1) the use of existing medical records that were collected for the purpose of diagnosis and treatment and not specifically for the purpose of this research may not be ideal; (2) Over reporting, underreporting, and errors in reporting results in misclassification; (3) Lack of access to the details of all patient records (data including type of AMI, body mass index, blood pressure, past medical history, blood urea nitrogen, creatinine) precludes more detailed results; (4) On the other hand, a limitation of the present study was that we relied on central station monitoring for meteorological factors instead of measurements of exposure to environmental variables; (5) Usually in these hospitals, a wide range of patients with ACS and similar diseases are recorded in health information system. So we gathered all of them for the specified interval; (6) Another limitation to consider is that patients who died before reaching the hospital or patients that were not admitted to any hospital (outpatients) may have been excluded, thus underrepresenting the sample; (7) the possibility of having admitted patients from other provinces to this study could not be verified. Thus, caution must be exercised when interpreting the study results.
Nevertheless, several unique features of this study are the large sample size; we relied on central station monitoring for meteorological factors instead of measurements of exposure to environmental variables this provided us the dependent variables (meteorological data) data that was unbiased with regards to outcome of this study; and lastly using these data bases allowed us to answer research questions and generate new hypothesis for testing in future studies without the exorbitant cost of planning a prospective study.
Recommendation
We recommended that more detailed studies be conducted to verify the present results by other investigators. More detailed results about the incidence of ACS regarding to seasonal changes can help us in planning and thus potentially reducing ACS. Future studies with samples from different populations and also longitudinal designs are suggested to verify the findings of this study. Importantly, this study provides useful data that can be applied to future studies. Future studies are recommended that incorporate more detailed patients information (such as type of ACS, body mass index, blood pressure, past medical history, blood urea nitrogen, creatinine), wider climate areas (such as warm and dry; cold and dry).
Conclusion
Climate changes were found to be significantly associated with ACS. Especially from cold weather to hot weather in March, April and May. Therefore, emergency treatment service personnel should be more vigilant and fully prepared in March, April, and May for an increase in ACS patient admissions.
Ethical approval
The study was approved (Code: IR.MAZUMS.REC.96-10232) by the Ethics Committee of Mazandaran University of Medical Sciences, Sari, Iran, pursuant to its code of ethics, including assured confidentiality of all patient information.
Competing interests
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
Authors’ contributions
HShN, YHC, RN, and AHG were on the management committee. HSHN, ESF, AHG, AKH, RP, and AY were on the scientific committee. RP, SPSh, HSHN, AKH, FA, and ESF were responsible for data interpretation and writing the report. RP, SPSh, and AKH did the statistical analysis. HShN, AHG, AY, RN, and RP were on the writing committee. HShN, AY, ESF, YHC, FA, AKH, and SPSh reviewed and revised the manuscript. All authors reviewed the manuscript.
Acknowledgments
This project was an inter-university collaboration and was supported by Mazandaran University of Medical Sciences, Taylor’s University and University of California San Francisco. We want to hereby extend our sincere gratitude to the all of the authorities of the heart center who helped to make this research possible.
References
- Sharif Nia H, Sivarajan-Froelicher E, Haghdoost AA, Moosazadeh M, Huak-Chan Y, Farsavian AA, et al. The estimate of average age at the onset of acute myocardial infarction in Iran: a systematic review and meta-analysis study. ARYA Atheroscler 2018;14(5):225-32. doi: 10.22122/arya.v14i5.1739. [Crossref]
- Sharif Nia H, Haghdoost AA, Nazari R, Bahrami N, Soleimani MA, Pormand K. Relationship of risk factors and ST segment changes with symptoms of acute coronary syndrome. Koomesh 2013;15(1):46-53.
- Honda T, Fujimoto K, Miyao Y. Influence of weather conditions on the frequent onset of acute myocardial infarction. J Cardiol 2016;67(1):42-50. doi: 10.1016/j.jjcc.2015.02.013. [Crossref]
- Moschos N, Christoforaki M, Antonatos P. Seasonal distribution of acute myocardial infarction and its relation to acute infections in a mild climate. Int J Cardiol 2004;93(1):39-44.
- Sen T, Astarcioglu MA, Asarcikli LD, Kilit C, Kafes H, Parspur A, et al. The effects of air pollution and weather conditions on the incidence of acute myocardial infarction. Am J Emerg Med 2016;34(3):449-54. doi: 10.1016/j.ajem.2015.11.068. [Crossref]
- Kriszbacher I, Bodis J, Csoboth I, Boncz I. The occurrence of acute myocardial infarction in relation to weather conditions. Int J Cardiol 2009;135(1):136-8. doi: 10.1016/j.ijcard.2008.01.048. [Crossref]
- Goggins WB, Chan EY, Yang CY. Weather, pollution, and acute myocardial infarction in Hong Kong and Taiwan. Int J Cardiol 2013;168(1):243-9. doi: 10.1016/j.ijcard.2012.09.087. [Crossref]
- Patel NJ, Pant S, Deshmukh AJ, Nalluri N, Badheka AO, Shah N, et al. Seasonal variation of acute myocardial infarction related hospitalizations in the United States: perspective over the last decade. Int J Cardiol 2014;172(3):e441-2. doi: 10.1016/j.ijcard.2013.12.319. [Crossref]
- Ogbebor O, Odugbemi B, Maheswaran R, Patel K. Seasonal variation in mortality secondary to acute myocardial infarction in England and Wales: a secondary data analysis. BMJ Open 2018;8(7):e019242. doi: 10.1136/bmjopen-2017-019242. [Crossref]
- Culic V. Seasonal distribution of acute myocardial infarction: a need for a broader perspective. Int J Cardiol 2006;109(2):265-6. doi: 10.1016/j.ijcard.2005.03.074. [Crossref]
- Radisauskas R, Bernotiene G, Baceviciene M, Ustinaviciene R, Kirvaitiene J, Kranciukaite-Butylkiniene D. Trends of myocardial infarction morbidity and its associations with weather conditions. Medicina (Kaunas) 2014;50(3):182-9. doi: 10.1016/j.medici.2014.08.003. [Crossref]
- Madrigano J, Mittleman MA, Baccarelli A, Goldberg R, Melly S, von Klot S, et al. Temperature, myocardial infarction, and mortality: effect modification by individual- and area-level characteristics. Epidemiology 2013;24(3):439-46. doi: 10.1097/EDE.0b013e3182878397. [Crossref]
- Messner T, Lundberg V, Wikstrom B. A temperature rise is associated with an increase in the number of acute myocardial infarctions in the subarctic area. Int J Circumpolar Health 2002;61(3):201-7.
- Morabito M, Modesti PA, Cecchi L, Crisci A, Orlandini S, Maracchi G, et al. Relationships between weather and myocardial infarction: a biometeorological approach. Int J Cardiol 2005;105(3):288-93. doi: 10.1016/j.ijcard.2004.12.047. [Crossref]
- Loomba RS. Seasonal variation in paroxysmal atrial fibrillation: A systematic review. J Atr Fibrillation 2015;7(5):1201. doi: 10.4022/jafib.1201. [Crossref]
- Rumana N, Kita Y, Turin TC, Murakami Y, Sugihara H, Morita Y, et al. Seasonal pattern of incidence and case fatality of acute myocardial infarction in a Japanese population (from the Takashima AMI Registry, 1988 to 2003). Am J Cardiol 2008;102(10):1307-11. doi: 10.1016/j.amjcard.2008.07.005. [Crossref]
- Spencer FA, Goldberg RJ, Becker RC, Gore JM. Seasonal distribution of acute myocardial infarction in the second National Registry of Myocardial Infarction. J Am Coll Cardiol 1998;31(6):1226-33.
- Gonzalez Hernandez E, Cabades O’Callaghan A, Cebrian Domenech J, Lopez Merino V, Sanjuan Manez R, Echanove Errazti I, et al. Seasonal variations in admissions for acute myocardial infarction. The PRIMVAC study. Rev Esp Cardiol 2004;57(1):12-9. [Spanish].
- Akioka H, Yufu K, Teshima Y, Kawano K, Ishii Y, Abe I, et al. Seasonal variations of weather conditions on acute myocardial infarction onset: Oita AMI Registry. Heart Vessels 2019;34(1):9-18. doi: 10.1007/s00380-018-1213-6. [Crossref]
- Fares A. Winter cardiovascular diseases phenomenon. N Am J Med Sci 2013;5(4):266-79. doi: 10.4103/1947-2714.110430. [Crossref]
- Lin GM, Li YH, Lin CL, Wang JH, Han CL. Seasonal variation in cardiac death of patients with angiographic coronary artery disease from the ET-CHD registry, 1997-2006. Int J Cardiol 2013;168(3):3090-2. doi: 10.1016/j.ijcard.2013.04.080. [Crossref]
- Grant WB, Bhattoa HP, Boucher BJ. Seasonal variations of US mortality rates: Roles of solar ultraviolet-B doses, vitamin D, gene exp ression, and infections. J Steroid Biochem Mol Biol 2017;173:5-12. doi: 10.1016/j.jsbmb.2017.01.003. [Crossref]
- Abrignani MG, Corrao S, Biondo GB, Renda N, Braschi A, Novo G, et al. Influence of climatic variables on acute myocardial infarction hospital admissions. Int J Cardiol 2009;137(2):123-9. doi: 10.1016/j.ijcard.2008.06.036. [Crossref]
- Goudarzian AH, Sharif Nia H, Jafari H, Jamali S, Badiee M, Sayemi Z, et al. Inpatient satisfaction with health system transformation project in mazandaran educational hospitals, Iran. Journal of Mazandaran University of Medical Sciences 2016;26(136):190-5. [Persian].
- Spielberg C, Falkenhahn D, Willich SN, Wegscheider K, Voller H. Circadian, day-of-week, and seasonal variability in myocardial infarction: comparison between working and retired patients. Am Heart J 1996;132(3):579-85.
- Wang H, Kakehashi M, Matsumura M, Eboshida A. Association between occurrence of acute myocardial infarction and meteorological factors. J Cardiol 2007;49(1):31-40. [Japanese].
- Wang H, Matsumura M, Kakehashi M, Eboshida A. Seasonal variations and the effect of atmospheric temperature on the incidence of coronary heart disease in Hiroshima, Japan. J Health Sci Hiroshima Univ 2005;4(2):82-9. doi: 10.15027/16446. [Crossref]
- Fischer T, Lundbye-Christensen S, Johnsen SP, Schonheyder HC, Sorensen HT. Secular trends and seasonality in first-time hospitalization for acute myocardial infarction--a Danish population-based study. Int J Cardiol 2004;97(3):425-31. doi: 10.1016/j.ijcard.2003.10.026. [Crossref]
- Mahmoud KD, Lennon RJ, Ting HH, Rihal CS, Holmes DR Jr. Circadian variation in coronary stent thrombosis. JACC Cardiovasc Interv 2011;4(2):183-90. doi: 10.1016/j.jcin.2010.09.025. [Crossref]
- Isik T, Ayhan E, Uyarel H, Akkaya E, Ergelen M, Cicek G, et al. Circadian, weekly, and seasonal variation in early stent thrombosis patients who previously underwent primary percutaneous intervention with ST elevation myocardial infarction. Clin Appl Thromb Hemost 2013;19(6):679-84. doi: 10.1177/1076029612445918. [Crossref]
- Amiya S, Nuruki N, Tanaka Y, Tofuku K, Fukuoka Y, Sata N, et al. Relationship between weather and onset of acute myocardial infarction: can days of frequent onset be predicted? J Cardiol 2009;54(2):231-7. doi: 10.1016/j.jjcc.2009.05.011. [Crossref]
- Li QB, Sheng L, He Y. The effect of climatic factors on the onset of acute myocardial infarction. Zhonghua Hu Li Za Zhi 1997;32(11):621-4. [Chinese].
- Matthews CE, Freedson PS, Hebert JR, Stanek EJ 3rd, Merriam PA, Rosal MC, et al. Seasonal variation in household, occupational, and leisure time physical activity: longitudinal analyses from the seasonal variation of blood cholesterol study. Am J Epidemiol 2001;153(2):172-83.
- Khaw KT. Temperature and cardiovascular mortality. Lancet 1995;345(8946):337-8.
- Meier CR, Jick SS, Derby LE, Vasilakis C, Jick H. Acute respiratory-tract infections and risk of first-time acute myocardial infarction. Lancet 1998;351(9114):1467-71.
- Sunyer J, Ballester F, Tertre AL, Atkinson R, Ayres JG, Forastiere F, et al. The association of daily sulfur dioxide air pollution levels with hospital admissions for cardiovascular diseases in Europe (The Aphea-II study). Eur Heart J 2003;24(8):752-60.
- Isik T, Ayhan E, Uyarel H, Gunaydin ZY, Bektas O, Karagoz A. The Relation between Seasonal Variation and Mortality in Patients with ST Elevation Myocardial Infraction. Acta Med Mediterr 2015;31:561-7.
- Stewart S, Keates AK, Redfern A, McMurray JJV. Seasonal variations in cardiovascular disease. Nat Rev Cardiol 2017;14(11):654-64. doi: 10.1038/nrcardio.2017.76. [Crossref]
- Goerre S, Egli C, Gerber S, Defila C, Minder C, Richner H, et al. Impact of weather and climate on the incidence of acute coronary syndromes. Int J Cardiol 2007;118(1):36-40. doi: 10.1016/j.ijcard.2006.06.015. [Crossref]
- Aylin P, Morris S, Wakefield J, Grossinho A, Jarup L, Elliott P. Temperature, housing, deprivation and their relationship to excess winter mortality in Great Britain, 1986-1996. Int J Epidemiol 2001;30(5):1100-8.
- Messner T, Lundberg V, Wikstrom B. The Arctic Oscillation and incidence of acute myocardial infarction. J Intern Med 2003;253(6):666-70.
- Lee JH, Chae SC, Yang DH, Park HS, Cho Y, Jun JE, et al. Influence of weather on daily hospital admissions for acute myocardial infarction (from the Korea Acute Myocardial Infarction Registry). Int J Cardiol 2010;144(1):16-21. doi: 10.1016/j.ijcard.2009.03.122. [Crossref]
- Chang CL, Shipley M, Marmot M, Poulter N. Lower ambient temperature was associated with an increased risk of hospitalization for stroke and acute myocardial infarction in young women. J Clin Epidemiol 2004;57(7):749-57. doi: 10.1016/j.jclinepi.2003.10.016. [Crossref]
- Panagiotakos DB, Chrysohoou C, Pitsavos C, Nastos P, Anadiotis A, Tentolouris C, et al. Climatological variations in daily hospital admissions for acute coronary syndromes. Int J Cardiol 2004;94(2-3):229-33. doi: 10.1016/j.ijcard.2003.04.050. [Crossref]
- Ministry of Health, Labour and Welfare. Vital statistics of Japan. Available from: https://www.mhlw.go.jp/english/database/db-hw/dl/81-1a2en.pdf. Accessed 2016.
- Danet S, Richard F, Montaye M, Beauchant S, Lemaire B, Graux C, et al. Unhealthy effects of atmospheric temperature and pressure on the occurrence of myocardial infarction and coronary deaths. A 10-year survey: the Lille-World Health Organization MONICA project (Monitoring trends and determinants in cardiovascular disease). Circulation 1999;100(1):E1-7.
- Ku CS, Yang CY, Lee WJ, Chiang HT, Liu CP, Lin SL. Absence of a seasonal variation in myocardial infarction onset in a region without temperature extremes. Cardiology 1998;89(4):277-82. doi: 10.1159/000006800. [Crossref]
- Kysely J, Pokorna L, Kyncl J, Kriz B. Excess cardiovascular mortality associated with cold spells in the Czech Republic. BMC Public Health 2009;9:19. doi: 10.1186/1471-2458-9-19. [Crossref]
- Nayha S. Environmental temperature and mortality. Int J Circumpolar Health 2005;64(5):451-8.
- Gutierrez Loyola A, Druyet Castillo D, Oramas Dominguez I, Veliz Martinez PL. Infarto de miocardio agudo en Cuba. Situación actual. Rev Cub Med Int Emerg 2010;9(1):1638-48.
- Rivero A, Bolufe J, Ortiz PL, Rodriguez Y, Reyes MC. Influence of climate variability on acute myocardial infarction mortality in Havana, 2001-2012. MEDICC Rev 2015;17(2):14-9.
- Hodzic E, Perla S, Iglica A, Vucijak M. Seasonal Incidence of Acute Coronary Syndrome and Its Features. Mater Sociomed 2018;30(1):10-4. doi: 10.5455/msm.2018.30.10-14. [Crossref]
- Saligheh M, Bayat A, Behboudi H, Zakeri A, Jamali F. Spatial dispersion of climatic factors in North and central basin of Iran using statistical models. Journal of Geographical Sciences 2015;15(36):157-79.
- Daheshvar T, Danehkar A, Ale Sheikh AA, Ahmadian R. Identifying and Locating the Suitable Urban Development Spots with Application Criteria of Ecosystem (Case Study: Mahmood Abad Township, Mazandaran Province). Town and Country Planning 2013;5(1):155-79. [Persian].